Please note: This page is intended for healthcare professionals only. It is designed as a general educational guide and does not replace local guidance, senior clinical advice, or individual clinical judgement. Patients should not use this page as medical advice and should seek advice from an appropriate healthcare professional.
Testicular Torsion
Twisting of the spermatic cord → acute interruption of testicular blood supply → time-critical ischaemia and possible testicular loss.
Immediate priorities
Acute severe testicular pain should be assumed to be torsion until proven otherwise.
This is time-critical: notify a senior urologist urgently, keep the patient NBM, provide analgesia, and do not delay surgery for imaging if clinical suspicion is high.
Background
There are 2 types of torsion:
- Intravaginal torsion: Most common type. Occurs when the testis rotates within the tunica vaginalis. Classically in pubertal boys (12–18 years). Associated with bell-clapper deformity (failure of normal posterior anchoring → freely mobile testis).
- Extravaginal torsion: Seen mainly in neonates. Entire testis and tunica vaginalis twist together outside the tunica vaginalis. Often perinatal, presents with a firm, hard, non-tender scrotal mass. Usually unsalvageable due to delayed presentation.
Epidemiology: Bimodal peaks: Neonatal period (extravaginal) and Puberty (12–18 years) (intravaginal). Torsion can occur at any age, although it is rare in older patients.
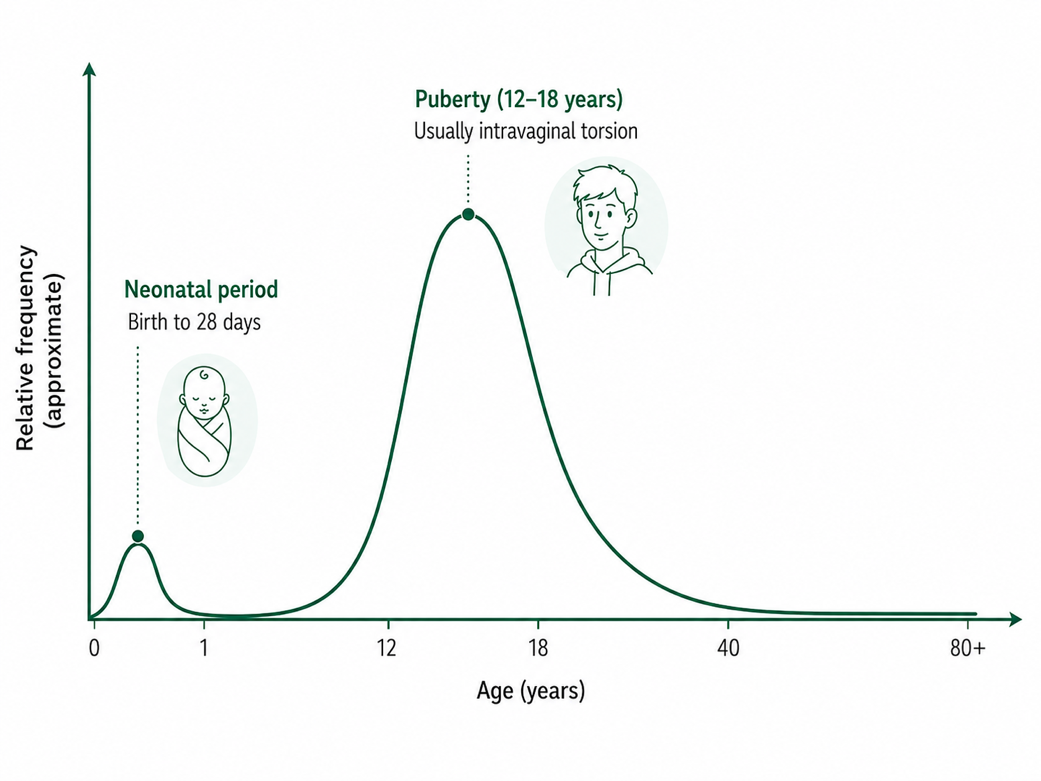 Schematic age-related frequency of testicular torsion
Schematic age-related frequency of testicular torsion
History
- Sudden onset severe unilateral testicular or lower abdominal pain
- Pain often <6 hrs
- Swelling develops quickly
- Nausea/vomiting common
- Pain not relieved by scrotal elevation (negative Prehn's sign, but unreliable)
- No LUTS (helps differentiate from epididymo-orchitis)
Assessment
- History: acute onset, severity, age (peak 12-18 years but may affect any age)
- Examination:
- Swollen, firm, high riding testis with transverse lie
- Loss of cremasteric reflex (not diagnostic, is a late sign)
- Scrotal erythema/oedema may occur as a late sign
- Compare to contralateral side
TWIST Score (Testicular Workup for Ischaemia and Suspected Torsion)
Useful triage tool, not a replacement for senior review.
Features
- Testicular swelling → 2 points
- Hard testis → 2 points
- Absent cremasteric reflex → 1 point
- Nausea/vomiting → 1 point
- High-riding testis → 1 point
Interpretation
0–2 = Low risk → consider alternative diagnoses; USS if needed
3–4 = Intermediate risk → urgent senior review; likely USS if available without delay
5–7 = High risk → treat as torsion → immediate surgical exploration
Diagnosis
- Diagnosis is made based on clinical examination (clinical diagnosis)
- In the UK setting, clinical suspicion alone mandates exploration; imaging should not delay surgery
- Bloods not routinely required unless concern for sepsis or other pathology
- Urine dip
- Doppler ultrasound only if diagnosis uncertain (reduced/absent arterial flow)
- Scrotal exploration is both diagnostic and therapeutic
Management
- Immediate senior (SpR/consultant) notification
- Keep NBM, IV access, analgesia
- Scrotal exploration if torsion cannot be confidently excluded
- Perform bilateral orchidopexy if viable → or orchidectomy if non-viable
- Time to salvage
- < 6 hrs → 90–100% salvage
- 12 hrs → ~50%
- > 24 hrs → < 10%
Patient Information leaflet → BAUS patient information leaflet for scrotal exploration for suspected torsion of testis
GIRFT Guidelines
- A national pathway developed by a multi-disciplinary group (paediatric surgeons, urologists, radiologists, emergency physicians, etc) under the GIRFT Children & Young People programme.
- It responds to findings that children and young people presenting with acute scrotal pain are sometimes undergoing surgery too late (leading to testicular loss) due to delays at various stages (referral, transfer, diagnosis).
NB! It is intended as guidance to streamline care, not a rigid rule-book—clinical judgement remains essential.
Read full guidance HERE
RED FLAGS
- Acute severe testicular pain - assume torsion until proven otherwise
- Time-critical
- High-riding testis with transverse lie
- Loss of cremasteric reflex (not diagnostic, is a late sign)
- Do NOT delay surgery for imaging if clinical suspicion is high