Overview
A urethral stricture is a narrowing of the urethral lumen caused by scar tissue formation. This may result in progressive bladder outlet obstruction and subsequent recurrent infection, urinary retention and, in severe cases, upper tract deterioration.
Urethral strictures affect approximately 0.6% of men and are uncommon in women. Although they may occur at any age, they are more commonly diagnosed in older men.
Most strictures occur within the bulbar urethra.
Stricture Location
Urethral strictures are broadly divided into anterior and posterior strictures.
The majority of strictures occur within the anterior urethra. Stricture location is important because it influences both symptoms and treatment options.
Anterior strictures
involve:
- Meatal or submeatal (fossa navicularis)
- Penile urethra
- Bulbar urethra
Common causes include:
- Idiopathic
- Instrumentation (prior urological surgery, catheterisation, sounding etc.)
- Balanitis xerotica obliterans (BXO)
- Infection (particularly after STI)
- Trauma (straddle injury, penile trauma)
Posterior strictures
involve:
- Membranous urethra
- Prostatic urethra
- Bladder neck
- Bladder neck contracture is not technically a urethral stricture but is commonly considered alongside posterior stricture disease
Common causes include:
- Pelvic fracture urethral injury (PFUI)
- Prostate surgery
- Pelvic radiotherapy
When Should I Suspect a Stricture?
- ✓Gradually worsening weak stream
- ✓Spraying or split urinary stream
- ✓Obstructive LUTS or bladder outflow obstruction with a small prostate
- ✓Previous catheterisation or instrumentation
- ✓Previous pelvic trauma
- ✓BXO (could have history of circumcision)
- ✓Younger men presenting with LUTS, especially if there is a history of previous hypospadias surgery or points mentioned above
On-Call Relevance
The immediate priority is management of the acute problem. Definitive stricture treatment is usually arranged electively.
Common stricture-related presentations include:
- Acute urinary retention
- Difficult catheterisation
- Recurrent urinary tract infection
Assessment
Patients with suspected urethral stricture disease should undergo a standard LUTS assessment as described in the LUTS section.
Particular attention should be paid to:
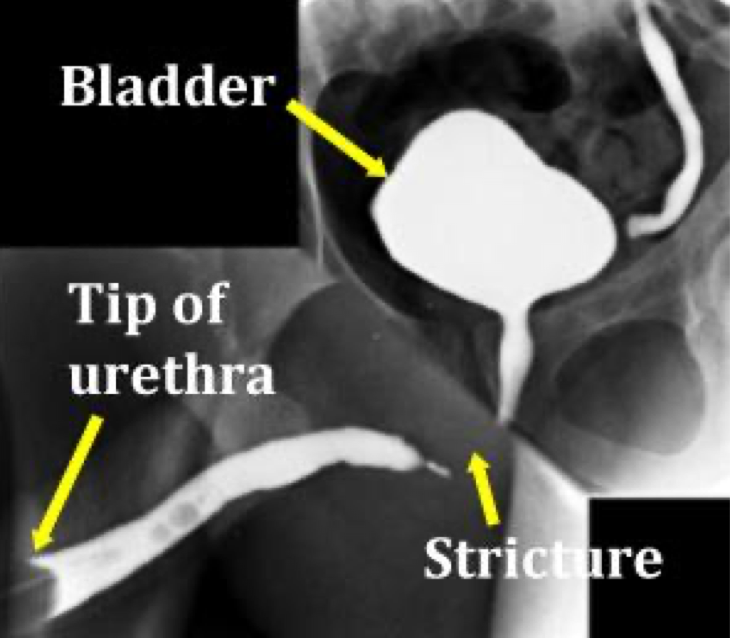
RUG of bulbar stricture
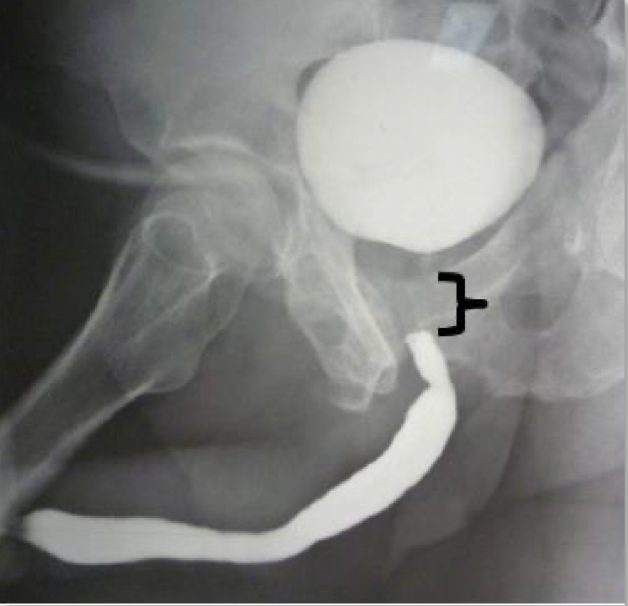
RUG of posterior urethral disruption
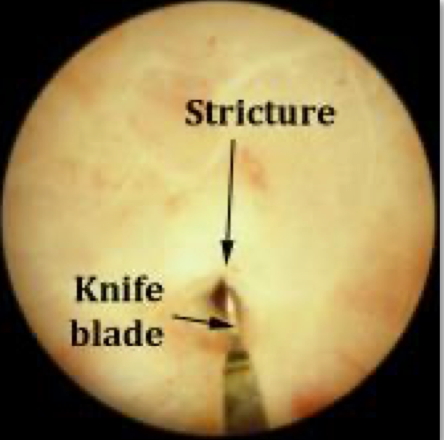
Cystoscopic view of stricture with pinhole lumen during surgery
1
History of
- Previous catheterisation and endoscopic surgery
- Pelvic trauma
- Previous radiotherapy
- Recurrent UTI’s
- Spraying stream
- Previous stricture treatment
- Symptoms suggestive of BXO
2
During examination
- External genitalia assessment
- Examine perineum – look for scars and perineal abnormalities (eg. fistula)
3
Investigations
Investigations for strictures are usually done electively in outpatient setting. These include:
- Urinalysis +/- MSU
- Uroflowmetry and post-void residual (PVR)
- May identify poor bladder emptying and chronic retention.
- Renal Function
- Check if retention or upper tract obstruction is suspected.
- Upper Tract Imaging
- Consider renal tract ultrasound in patients with:
- Chronic retention
- Elevated creatinine
- Recurrent infections
- Flexible Cystoscopy
- Allows direct visualisation of the urethra and may identify:
- Stricture location
- Severity
- Associated pathology
- Retrograde Urethrogram (RUG)
- Often considered the gold standard imaging investigation for urethral stricture disease.
- RUG is particularly useful when planning surgery and may define:
- It may also be used in the assessment of urethral trauma.
Difficult Catheterisation
Urethral strictures are a common cause of difficult catheterisation. If patient is known to have a stricture or you suspect it, then the principles are:
- Never force a catheter!
- Use a small diameter catheter (eg. 12Fr)
- Use ample lubrication
- Seek senior help EARLY if resistance is encountered
- Repeated traumatic attempts may worsen the stricture and create false passages
Further information is available in the Difficult Catheterisation section.
Management Principles
Management depends on:
- Stricture length
- Stricture location
- Previous treatments
- Patient factors
Short, uncomplicated strictures may be suitable for endoscopic treatment, whereas recurrent or complex strictures often require reconstructive surgery.
See further information on procedures - HERE
A. Endoscopic Treatments
Urethral dilatation
Optical urethrotomy (DVIU)
Optilume drug-coated balloon
These may be appropriate for selected short strictures but recurrence remains common.
B. Reconstruction
This is usually done for patient with recurrent strictures suitable for surgery
Posterior strictures
These cases are often more complex and are typically managed in specialist reconstructive centres.
Anterior strictures
- Meatoplasty
- Urethroplasty
- Considered the gold standard curative treatment for recurrent or complex strictures
- This involves open reconstruction of the urethra and may utilise local tissue or buccal mucosal grafts.
C. Urinary diversion
In cases if restoration of normal urethral voiding may not be possible or desirable.
Long term urinary catheter (urethral or SPC)
Perineal Urethrostomy
Formation of ileal conduit
D. Stricture control
Intermittent self-dilatation (ISD)
For patients who prefer to avoid major surgery or are not suitable for definitive reconstruction they can manage their stricture with regular self-dilatation.
When to Refer?
Refer to urology if there is:
- Suspected urethral stricture disease
- BXO involving the urethral meatus
- Difficult catheterisation
- Persistent LUTS despite treatment