Manual bladder washout is a procedure used to clear the bladder of clots or debris. It involves instilling and aspirating sterile saline to maintain catheter patency.
Indications for a bladder washout
- Clot retention
- Persistent haematuria and/or haematuria with clots
- Catheter blockage
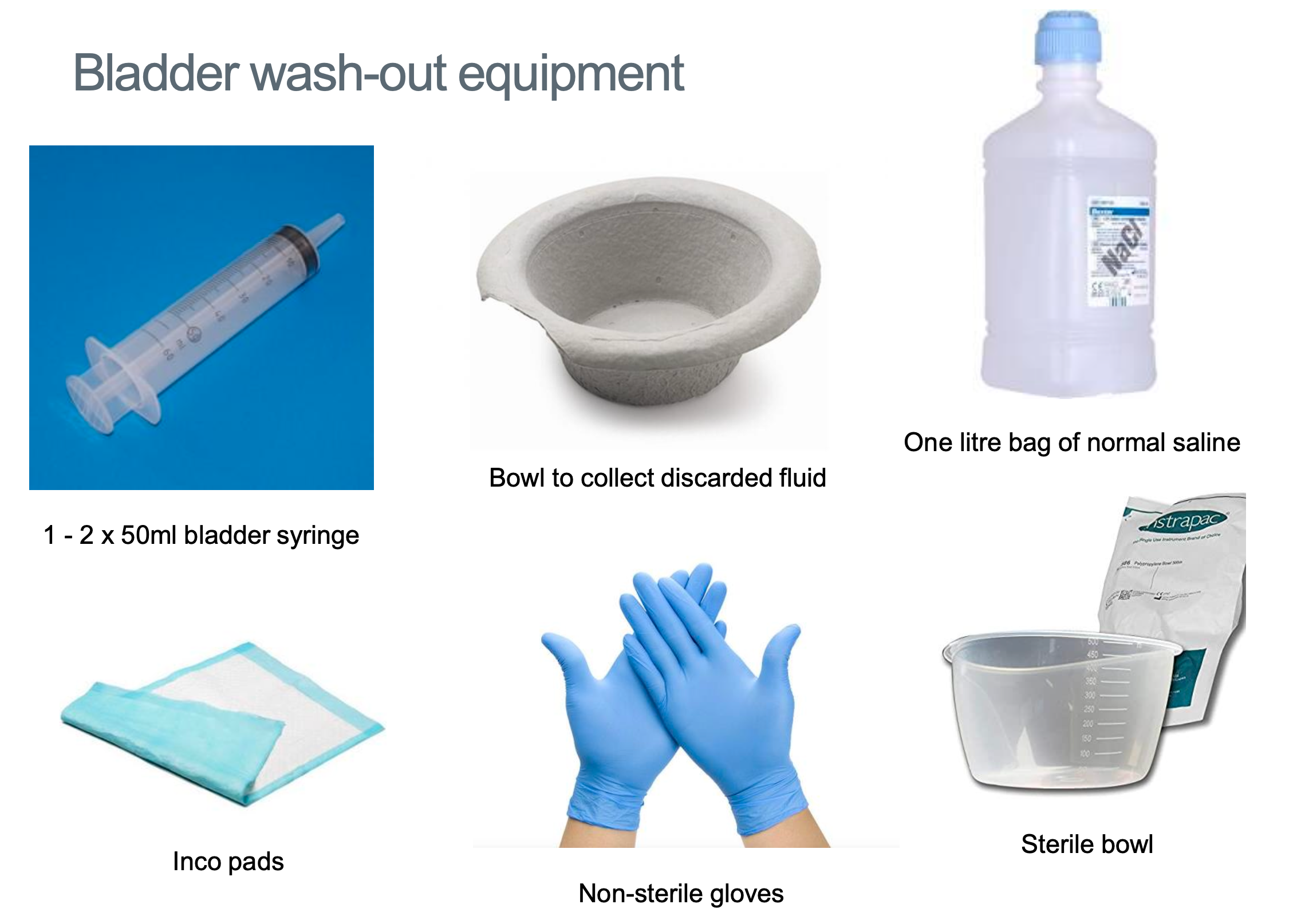
Equipment Required
- Trolley
- 1L Bottle of 0.9% NaCl or Sterile Water (warm will be more comfortable)
- 1x Sterile bowl
- 1x bowl to discard aspirate & clots
- 50mL bladder tip syringe (catheter tip)
- Non-sterile gloves and apron
- New catheter bag
- Disposable bed pads
This is an ANTT procedure.
Preparation
- Wash hands and don an apron and gloves
- Place disposable incontinence pads underneath the patient
- Position the patient comfortably supine at either 0 or 45o
- Pour 1L NaCl into one sterile bowl and place the discard bowl nearby for waste
- If 3-way catheter stop irrigation or put a spigot into the 3rd channel
 Spigot
Spigot
Technique
- Disconnect the catheter bag
- Draw up 50mL NaCl into a bladder tip syringe and connect to the catheter outflow channel (middle channel)
- Gently instil 50mL NaCl into the bladder and withdraw – warn patient of potential discomfort
- Aspirate as much back into the syringe and discard into the discard bowl
- Repeat the process of instillation and withdrawal up to 1000mL or until the fluid aspirated is clear of clots / drains rose or clear effluent
- Reconnect the catheter bag and consider starting/resuming continuous bladder irrigation
- Document the procedure, difficulties and outcome
- Of note - patients may require serial bladder washouts, which may involve performing more than one per day.
Bladder washouts following urological surgery – should be done very gently!! Do not overdistend the bladder → risk of perforation
Troubleshooting during bladder washout
In some cases, the fluid cannot be aspirated after it is instilled. This may occur due to clots/debris blocking the tip of the catheter or because of a large and organised clot
If unable to aspirate fluid after instillation, then you can try:
- Check catheter placed correctly!
- Instil further fluid (up to 150mL total, but stop if there is pain!)
- Gently advance and rotate the catheter with the balloon inflated
- Change the catheter
If still not working discuss with Urology SpR
- Might need to consider imaging to assess for organised clot
- Patient might require trip to theatre
When should I ask for help?
- If a patient is requiring very frequent bladder washouts
- Significant haematuria
- Patient has signs of anaemia or looks unwell
- Any change in patient observations – low BP, increased HR
- Can’t clear blockage
- Post-operative patient with worsening pain or poor drainage