Please note: This page is intended for healthcare professionals only. It is designed as a general educational guide and does not replace local guidance, senior clinical advice, or individual clinical judgement. Patients should not use this page as medical advice and should seek advice from an appropriate healthcare professional.
Upper Tract Procedures
This is a very brief introduction into most common urological operations. The list below is not exhaustive of all urological operations, but the procedures an SHO will more commonly encounter.
⚠️ Postoperative care is procedure and patient-specific. Always read the operation note before taking any action. Instructions regarding catheters, drains, stents, antibiotics, anticoagulation, imaging, and follow-up may differ between patients.
Patient information leaflets
- Kidney procedures – HERE
- Ureter procedures – HERE
- Stone procedures – HERE
Stone Procedures
Ureteroscopy (URS – Rigid or Flexible)
- Endoscopic treatment of ureteric or renal stones using laser fragmentation (Ho:YAG or Thulium)
- Smaller fragments can be removed with a basket
- Ureteric stent may be left afterwards
- Usually day-case
- Risks:
- Common – LUTS, haematuria, retention, need for staged procedure
- Serious – injury to urinary tract including perforation, strictures, sepsis
Ureteric Stent (Insertion / Removal / Exchange)
- Internal tube placed between the kidney and bladder to maintain urinary drainage
- Commonly inserted for obstruction, infection, ureteric injury, or following surgery
- Available in different materials (polymer, silicone, metallic)
- Risks: stent symptoms (LUTS and loin pain), haematuria, misplacement, blockage
Follow-up must be arranged before discharge:
- Further surgery
- Change:
- Polymer / silicone stents – usually 3–6 monthly
- Metallic stents – longer dwell time, often can be annual
- Removal:
- If stent on strings – usually removed within 7 days by patient or depending on local pathways
- If no strings – removal via flexible cystoscopy under LA
PCNL – Percutaneous Nephrolithotomy
- Percutaneous tract from flank directly into kidney for large or complex stones
- Variants: Standard, Mini-PCNL, Ultra-mini
- May leave a nephrostomy or stent
- Usually inpatient 1–2 days
- Risks:
- Common – haematuria, future stone recurrence
- Serious – bleeding needing transfusion, pneumo/haemothorax, sepsis, surrounding organ injury
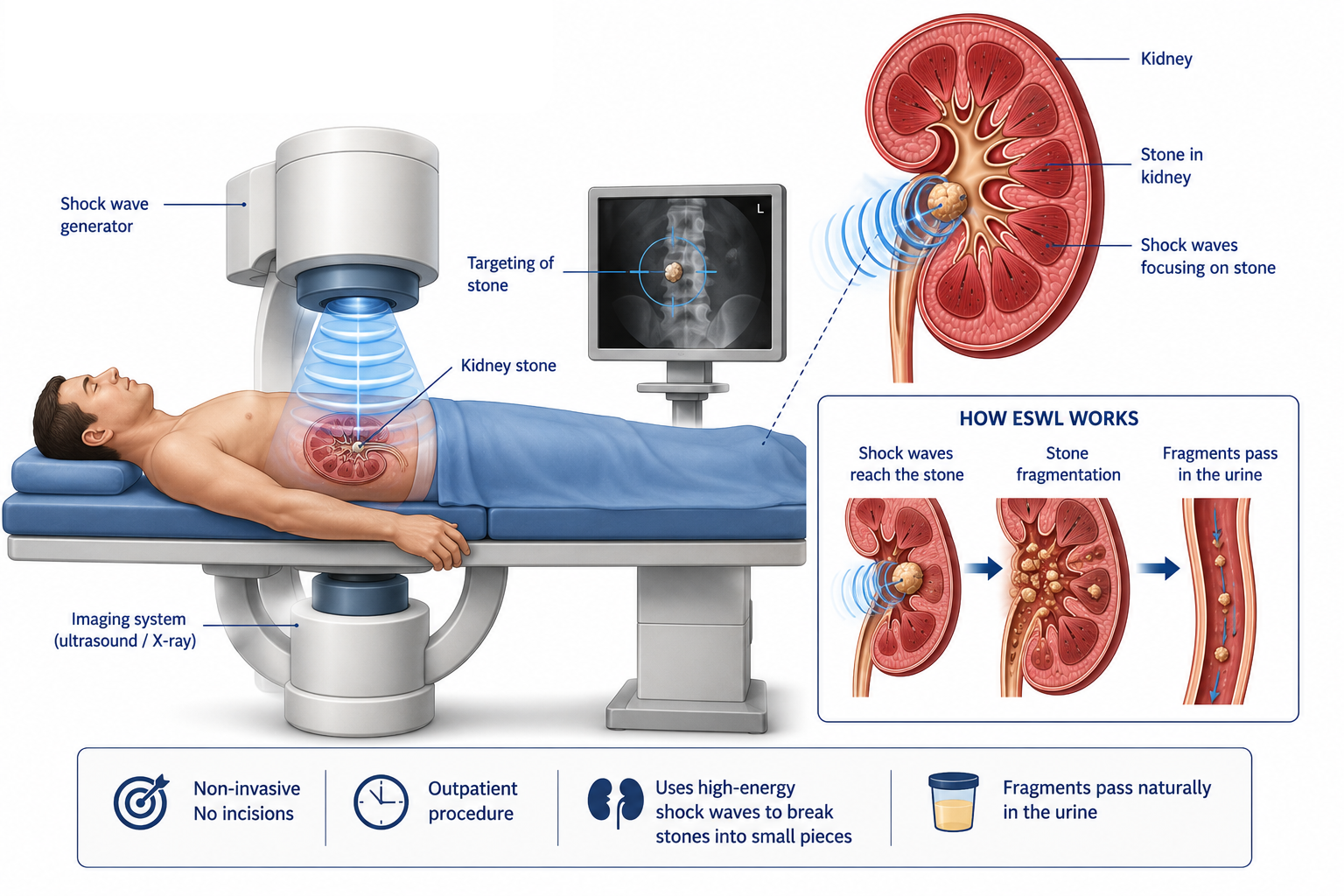
ESWL – Extracorporeal Shock Wave Lithotripsy
- Non-invasive shock-wave treatment (US/X-ray guided) to fragment renal or ureteric stones
- May not be appropriate for all stones
- Less favourable outcomes if stone is:
- Very dense (>1000 HU)
- Large (>2 cm)
- Increased skin-to-stone distance (>10 cm)
- Lower pole location
- Unfavourable anatomy
- May require repeat sessions; reduced efficacy in obesity, cystine/brushite stones, lower-pole stones
- Risks:
- Common – haematuria, pain during fragment passage, need for staged procedure
- Serious – steinstrasse, obstructing ureteric stone, UTI/sepsis, renal injury
- Contraindications: pregnancy, untreated UTI, anticoagulation/coagulopathy, significant AAA, infected obstruction (stent/nephrostomy instead)
Nephrostomy (IR-guided)
- Percutaneous drainage of kidney through the back to decompress an obstructed kidney
- Patients need clotting and G&S pre-operatively for new insertions
- Does patient need to be NBM before procedure? – practice varies between Radiology departments, please check locally.
- Nephrostomies are usually changed 3 monthly and first change needs to be booked before patient is discharged!
Cancer Procedures
Nephrectomy +/- Ureterectomy (Open / Laparoscopic / Robotic)
- Types:
- Radical nephrectomy – for renal cancer
- Radical nephro-ureterectomy – for ureteric / renal pelvic cancer. Post-operatively will have a catheter for longer period to allow bladder healing
- Simple nephrectomy – benign disease such as non-functioning kidney
- Kidney removed by making incision between two lap ports (this is not the same as conversion to open where a big incision is made in the flank or midline)
- Often patients go home in 1–2 days
Partial Nephrectomy (Open / Laparoscopic / Robotic)
- Removal of part of the kidney for small renal tumours = nephron-sparing
- Risks: post-op bleed, injury to surrounding organs (bowel / lung / liver / spleen / adrenal / pancreas), urine leak, positive margin
- Often go home within the next 1–2 days
Reconstructive Procedures
Pyeloplasty (Open / Lap / Robotic)
- Reconstruction of PUJ obstruction
- Excision of narrowed segment + re-anastomosis (e.g., Anderson–Hynes)
- JJ stent placed usually for 4–6 weeks