Please note: This page is intended for healthcare professionals only. It is designed as a general educational guide and does not replace local guidance, senior clinical advice, or individual clinical judgement. Patients should not use this page as medical advice and should seek advice from an appropriate healthcare professional.
Penile Cancer
Incidence & Overview
- Penile cancer is rare in Europe (≈ 1 per 100,000 men per year) but incidence is higher in parts of Africa, South America, and Asia
- Around 95% are squamous cell carcinoma (SCC)
- Most tumours arise on the glans or inner prepuce (foreskin)
- Associated with previous / current HPV infection (especially HPV 16 and 18) and these cases are biologically distinct from cases which are not HPV related
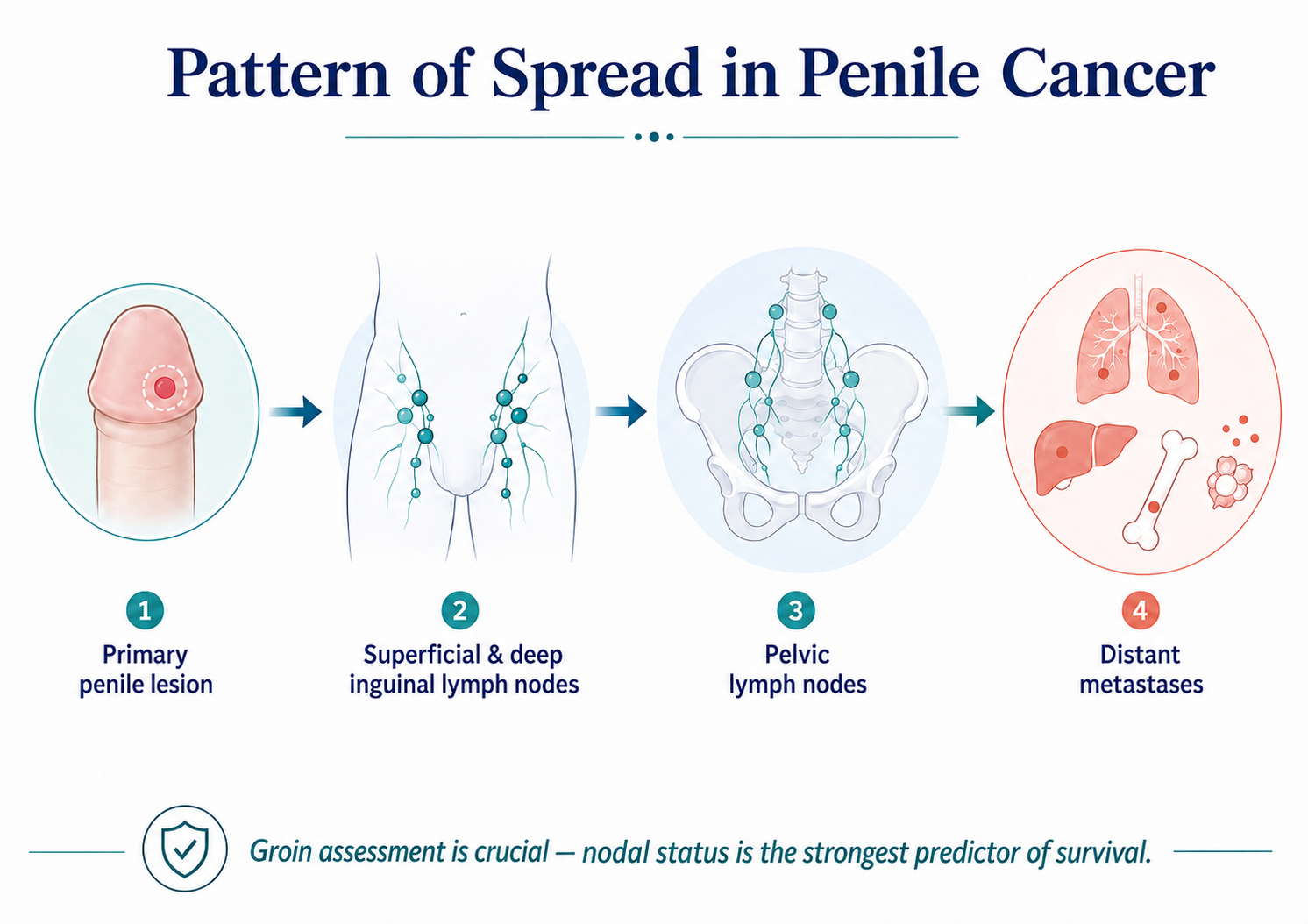
- Early diagnosis is crucial and spread to the inguinal lymph nodes is the strongest predictor of survival.
Risk Factors
✓Phimosis (key modifiable risk factor)
✓Chronic inflammatory conditions: lichen sclerosus (BXO), recurrent balanitis
✓HPV infection (30–50% of cases)
✓Smoking
✓Poor genital hygiene
✓Phototherapy with ultraviolet A light (PUVA)
Presentation
 Example of a meatal lesion
Example of a meatal lesion
- A lump, ulcer, fungating mass
- Wart-like/erythematous lesion may suggest PeIN (pre-cancerous change)
- Can be painless
- Secondary infection may mask underlying malignancy
Examination
- Always retract foreskin to examine the glans fully
- Attempt to unbury the penis if required
- Palpate inguinal lymph nodes — their status is the main prognostic determinant
- Note any meatal involvement — this may cause obstructive symptoms or urinary retention
NICE Suspected Cancer Referral Guidance
Consider a suspected cancer pathway referral for penile cancer in men if they have either:
- A penile mass or ulcerated lesion, where a sexually transmitted infection has been excluded as a cause, or
- A persistent penile lesion after treatment for a sexually transmitted infection has been completed.
Consider a suspected cancer pathway referral for penile cancer in men with unexplained or persistent symptoms affecting the foreskin or glans.
Investigations
- Histology
- Either through surgical excision of tumour or biopsy if the diagnosis is uncertain
- Imaging of primary tumour
- MRI penis – useful if:
- Concern about corporal invasion (T3 suspicion)
- Planning organ-preserving surgery and need to map tumour depth
- Lymph nodes
Lymph node staging can be done clinically and radiologically
cN0 (no palpable nodes)
- 20–25% still have occult micrometastases
- Intermediate/high-risk primaries (≥T1b) need dynamic sentinel lymph node biopsy (DSNB)
cN+ (palpable nodes)
- Confirm metastases with USS + FNAC
- Stage with CT chest/abdomen/pelvis or 18F-FDG-PET scan
NB! Advanced penile SCC can rarely be associated with paraneoplastic hypercalcaemia.
TNM Classification (UICC/AJCC 8th Ed)
UICC/AJCC 8th edition staging summary for penile cancer (From EAU–ASCO 2025 guideline).
| Stage |
Description |
| TPrimary Tumour |
| Tis |
PeIN (penile intra-epithelial neoplasia) |
| Ta |
Non-invasive verrucous carcinoma |
| T1 |
Invades subepithelial connective tissue |
| T1a |
No LVSI/PNI, not poorly differentiated |
| T1b |
LVSI/PNI or poor differentiation |
| T2 |
Invades corpus spongiosum (± urethra) |
| T3 |
Invades corpora cavernosa |
| T4 |
Invades adjacent structures (scrotum, prostate, pubic bone, etc.) |
cNClinical Nodes
cN0 – No palpable nodes
cN1 – One mobile unilateral node
cN2 – Multiple or bilateral mobile nodes
cN3 – Fixed inguinal mass or pelvic node involvement
pNPathological Nodes
pN1 – 1–2 unilateral nodes
pN2 – ≥3 unilateral or any bilateral
pN3 – Pelvic nodes or extranodal extension
MMetastasis
M0 – None
M1 – Distant disease
Quick Memory Aid
- T2 = spongiosum, T3 = cavernosum
- cN1 = one node, cN2 = multiple/bilateral, cN3 = fixed/pelvic
- PeIN = pre-cancerous changes → BAUS leaflet HERE
Follow-Up
- Highest risk of recurrence in first 24 months
- At each review: Inspect penile remnant or reconstruction, palpate inguinal nodes, monitor urinary/sexual function, lymphoedema
- Psychological and sexual rehabilitation support is important