Please note: This page is intended for healthcare professionals only. It is designed as a general educational guide and does not replace local guidance, senior clinical advice, or individual clinical judgement. Patients should not use this page as medical advice and should seek advice from an appropriate healthcare professional.
Haematuria: Visible vs Non-visible
Overview
Haematuria means the presence of blood in the urine. It may be visible with the naked eye or detected only on urine dipstick / microscopy.
For the SHO, the first step is not to diagnose the exact cause immediately, but to decide whether this is an acute presentation needing inpatient management or a stable presentation needing outpatient haematuria investigation.
This section will talk about general outlines of haematuria and non-acute management.
Haematuria types
Non-visible haematuria (nVH)
 Urine dipstick testing
Urine dipstick testing
- Non-visible haematuria (nVH), also known as microscopic haematuria, is the presence of blood in the urine that can only be detected on dipstick or microscopy. It is a common incidental finding that may require further investigations to assess for urological malignancy.
Defined as 1+ or more of blood on urine dipstick analysis
Trace haematuria is generally not considered significant
- Patients presenting with nVH are more commonly those with urinary tract stones and infections, but can still indicate a more sinister pathology, that in some cases, may warrant OP investigation (see NICE guidance).
Visible haematuria (VH)
- Visible (previously known as macroscopic or frank) haematuria is blood in the urine that can be seen with the naked eye. It often requires urgent investigation as it may indicate urological malignancy.
- Patients with visible haematuria often present to the emergency department. Visible haematuria may present alone or alongside other important symptoms. These patients will usually require an acute assessment by the on-call urology SHO.
- If patient has significant visible haematuria or clot retention – read HERE.
Causes
Common causes include:
- ✓Urological malignancy — bladder, renal, upper tract urothelial, prostate
- ✓Urinary tract infection – lower UTI / pyelonephritis / prostatitis
- ✓Renal tract stones
- ✓BPH / prostate bleeding
- ✓Recent instrumentation — catheter, cystoscopy, urology surgery
- ✓Trauma
- ✓Renal causes — glomerulonephritis, IgA nephropathy etc.; often associated with proteinuria
- ✓Radiation cystitis – for patient who had pelvic XRT
- ✓Exercise-induced haematuria (transient)
- ✓Decompression haematuria (following relief of chronic urinary retention)
- ✓Ketamine bladder – if history of illicit drug use; be especially vigilant in young patient presenting with visible haematuria and LUTS without evidence of infection
NICE Guidelines for referral to urology (NG12)
Visible haematuria
- Refer patients suspected cancer pathway referral (two-week wait referral)
- Patients 45 and above with unexplained visible haematuria in the absence of a urinary tract infection
- Refer patients 45 and above patients have persistent and/or recurrent visible haematuria after the successful treatment of a urinary tract infection
Non-visible haematuria
- Refer people aged 60 and above using a suspected cancer pathway referral (two-week wait) if they have unexplained non-visible haematuria and either:
- Dysuria
- Raised white cell count on a blood test
- Consider non-urgent referral for bladder cancer in people aged 60 and over with recurrent or persistent unexplained urinary tract infection.
Assessment
History
1Presenting complaint:
- Visible vs non-visible?
- If visible - how many instances?
- If nVH – how was this discovered?
- Any triggers or obvious causes of haematuria?
- Timing: throughout stream (bladder/upper tract) vs initial/terminal (prostatic/urethral)
- Presence of clots – suggests significant bleeding (further read HERE)
- Pain – think acute cause
- Suprapubic – cystitis, retention
- Loin pain – stones, pyelonephritis
- LUTS – storage and/or voiding symptoms
- Menstrual history in women
2Relevant past medical history:
- Previous surgery/instrumentation/trauma to the urinary tract
- History of pelvic irradiation, cyclophosphamide use (risk of bladder cancer)
- Anticoagulant/antiplatelet use
3Social history:
- Smoking status (key risk factor)
- Occupational exposure (dyes, rubber)
- Illicit drug use – especially ketamine
4Exclude transient causes:
- UTI (treat and repeat dipstick after 4 – 6 weeks)
- Menstruation
- Vigorous exercise
- ✓Painless visible haematuria (higher malignancy risk)
- ✓Recurrent visible haematuria
- ✓Associated weight loss or constitutional symptoms
- ✓Clot retention
- ✓Risk factors for urothelial cancer: smoking, occupational exposure, previous pelvic radiotherapy
- ✓Constitutional symptoms - weight loss, loss of appetite etc.
Examination
- Observations
- Abdominal examination — palpable bladder, loin tenderness, masses
- External genitalia
- DRE
- Assess hydration and haemodynamic stability
Investigations
General
- BP check (renal disease)
- Urine Dipstick: Confirm presence of blood (1+ or more). Check for protein (renal disease) or nitrites/leukocytes (infection)
- Bloods: U&Es, FBC, clotting if relevant
- PSA – if appropriate and after patient counselling
Specialist
Non-acute patients are usually seen in a “Haematuria clinic” or “One-stop clinic”.
If patients are referred for specialist investigations they will have both assessment of upper tracts (kidney, ureter) and lower tract (bladder, prostate, urethra).
1Flexible Cystoscopy
- Gold standard to examine bladder and urethra for malignancy
2Imaging
The choice of CT vs USS can vary between departments – check local pathways!
- CT Urogram – to assess for upper tract urothelial and renal malignancy
- Contrast CT with an excretory (urographic) phase
- Generally performed for all presenting with visible haematuria
- Able to detect ureteric filling defects suggestive of ureteric cancers
- Ultrasound of urinary tract
- Used more commonly for patients who have a low risk of upper tract/renal cancer with nVH
- May be considered as an alternative to CT
3Urine Cytology
- Not routinely recommended for initial investigation of VH or nVH due to low sensitivity
4Risk calculators
- IDENTIFY calculator — tool to estimate the probability of urinary tract cancer in patients presenting with haematuria. Helpful when counselling patients — available HERE
Management approach
First decide:
- Visible or non-visible?
- Painful or painless?
- Is the patient acutely unwell or obstructed?
|
Visible or non-visible?
|
Visible haematuria carries a higher risk of malignancy
|
|
Painful or painless?
|
Pain suggests acute causes:
- DDx – ureteric stone, infection, retention or trauma.
Painless:
- Visible haematuria – malignancy unless proven otherwise
- Non-visible haematuria – should be investigated as malignancy if persistent (see NICE guidance below)
|
|
Clots or retention?
|
Clots can obstruct the bladder outlet and need urgent catheterisation + bladder washout.
|
|
Septic, obstructed or unstable?
|
These patients need urgent escalation and acute management
|
Key message: painful haematuria usually suggests acute cause; painless visible haematuria needs cancer-pathway investigation unless there is a clear benign explanation.
PAINFUL haematuria
Think of acute causes and manage accordingly:
- Loin pain → ureteric stone / pyelonephritis
- Dysuria, fever, rigors → UTI / pyelonephritis / sepsis
- Suprapubic pain with clots and poor catheter drainage → clot retention (read HERE)
- Recent trauma/instrumentation → traumatic bleeding
Treat the underlying cause, resuscitate if needed, give antibiotics if infection, and escalate early if septic, obstructed, bleeding heavily or in retention.
PAINLESS haematuria
Painless visible haematuria is malignancy until proven otherwise.
If the patient is stable and well, is passing urine and haematuria is not significant, this is usually investigated as an outpatient through a Haematuria clinic.
Otherwise – if patient has significant haematuria, clot retention or is unwell – they will require inpatient admission + 3-way catheter and bladder washout. Read further management – HERE
When is haematuria considered "significant" for admission?
Non-visible haematuria = doesn’t require hospital admission.
- If incidental – repeat dipstick in 4-6 weeks, refer to Urology as per NICE guidance.
Visible haematuria = depends on the colour
- Light / pink / see-through = doesn’t require acute treatment; can be discharged with safety netting advice and investigated as outpatient
- Brown / coca-cola = old haematuria
- Maroon / merlot / fresh / clots = significant, and requires acute treatment – read further HERE
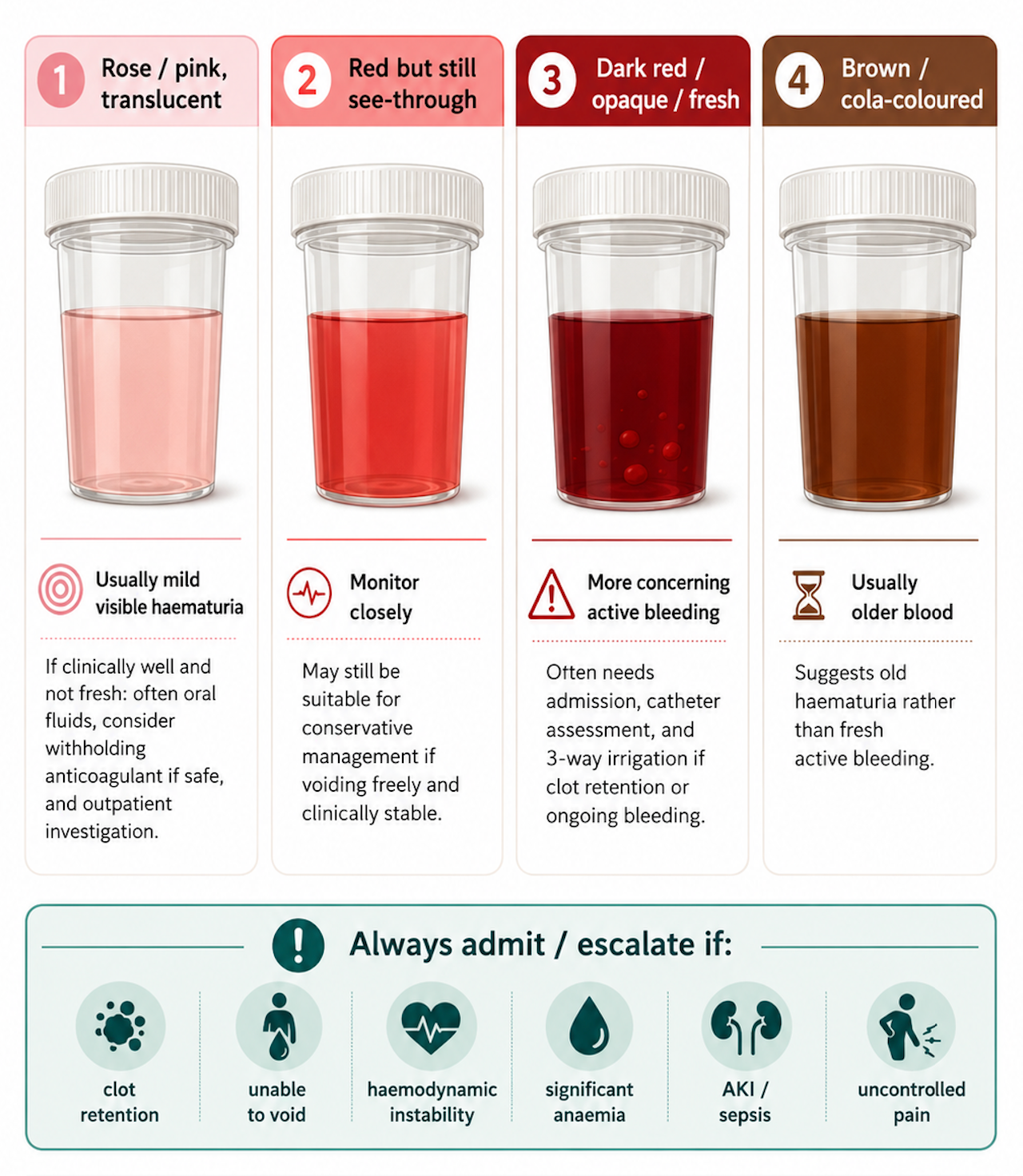 Grades of visible haematuria
Grades of visible haematuria
- Painful haematuria = think acute cause, needs urgent investigations
- Visible haematuria = cancer until proven otherwise, unless strong evidence of an alternative explanation
- If patient has incidental finding of nVH on dipstick – advise treating any possible cause and repeat dipstick with GP in 6 weeks. If still persistent then GP can refer patient as per NICE guidance.
- If ANY doubt = speak with Urology SpR/consultant
References
- NICE Guideline [NG12]. Suspected cancer: recognition and referral. 2015 (updated 2023).
- BAUS & The Renal Association. Joint Consensus Statement on the Initial Assessment of Haematuria. 2008.
- BAUS Consensus Document for the Management of Visible Haematuria
- IDENTIFY Risk Calculator – BURST Urology: HERE
- Khadhouri S, et al. The IDENTIFY Study: Developing a risk calculator for urinary tract cancer. Trends in Urology