Please note: This page is intended for healthcare professionals only. It is designed as a general educational guide and does not replace local guidance, senior clinical advice, or individual clinical judgement. Patients should not use this page as medical advice and should seek advice from an appropriate healthcare professional.
Torsion of Testicular Appendage
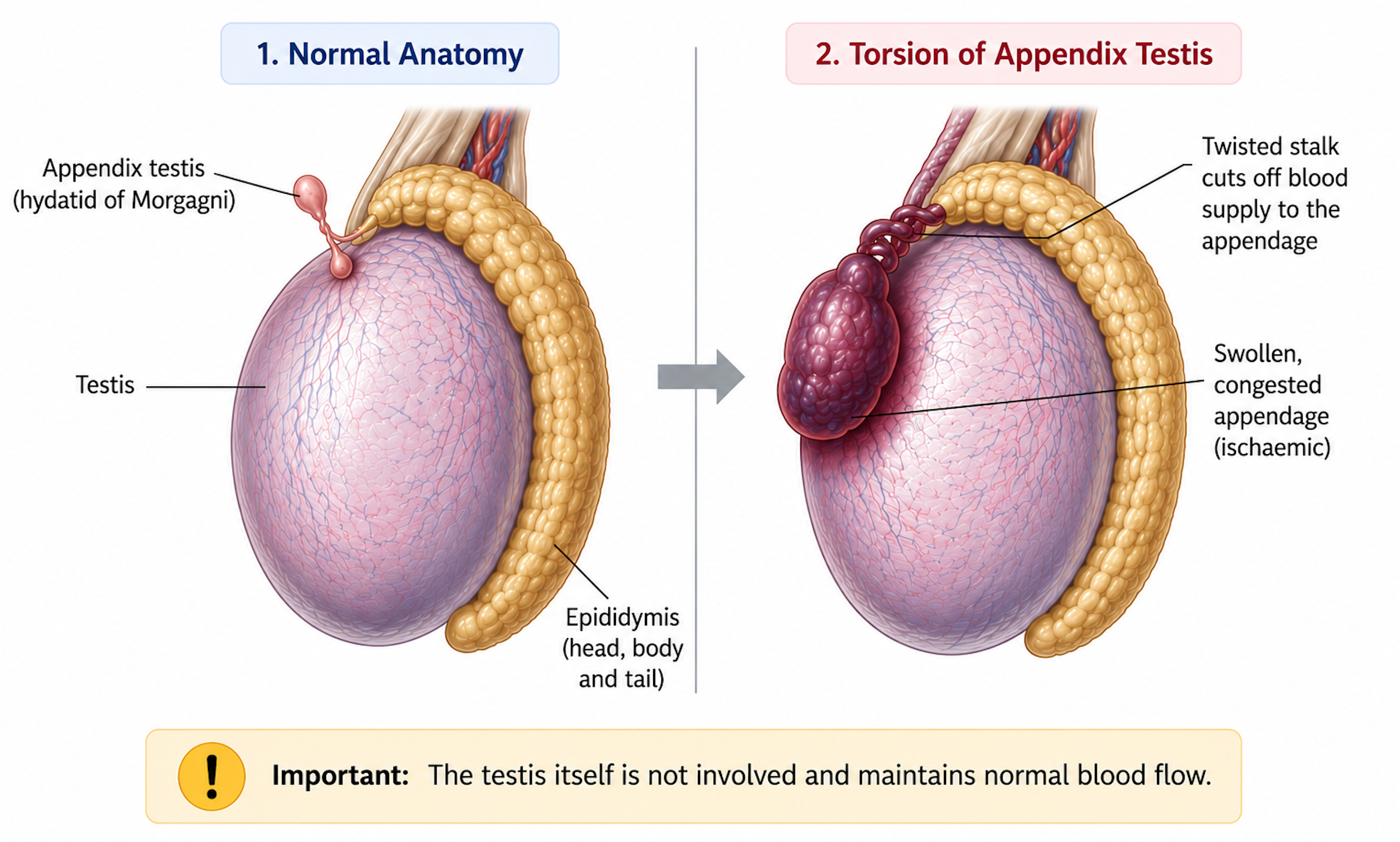
Torsion of the appendix testis or appendix epididymis (hydatid of Morgagni) — embryological remnants of the Müllerian and Wolffian ducts. Mimics testicular torsion but is benign and self-limiting.
 Torsion of appendix testis
Torsion of appendix testis
Epidemiology
- Most common in boys aged 7–12 years
- Much less common in infants and after late teens
- Accounts for ~40–60% of acute scrotum cases in prepubertal boys
Presentation
- Localised pain at the superior pole of the testis
- Tender paratesticular nodule at the upper testis/epididymis
- Cremasteric reflex usually preserved (helps differentiate from true torsion)
- Blue-dot sign (small blue/black spot through scrotal skin) – pathognomonic, but seen in ~20% of cases only
- Systemically well; no urinary symptoms
Assessment
- Pain is more localised rather than diffuse
- Testis typically not high-riding or horizontal
- Cremasteric reflex normally intact
- Less severe systemic upset (vomiting less common)
However — can still be difficult to distinguish clinically from testicular torsion.
Diagnosis
- Diagnosis based on clinical examination (clinical diagnosis)
- Doppler ultrasound may show normal testicular blood flow (if available and does not delay assessment)
If any doubt — treat as testicular torsion and proceed to surgical exploration.
Management
- Conservative treatment (if diagnosis certain)
- Bed rest
- Scrotal support/elevation
- NSAIDs and simple analgesia
- Usually resolves within 1 week
- Surgical exploration required if:
- Diagnosis uncertain
- Examination suggests possible testicular torsion
- Pain severe or persistent despite analgesia
Red Flags
- Worsening pain or clinical deterioration
- It can be clinically very difficult to distinguish appendage torsion from true testicular torsion
- If any doubt regarding the diagnosis → treat as testicular torsion and organise urgent surgical review/exploration