Please note: This page is intended for healthcare professionals only. It is designed as a general educational guide and does not replace local guidance, senior clinical advice, or individual clinical judgement. Patients should not use this page as medical advice and should seek advice from an appropriate healthcare professional.
Cauda Equina Syndrome & Metastatic Spinal Cord Compression
Cauda equina syndrome (CES) and metastatic spinal cord compression (MSCC) are neurological emergencies that often present with urinary symptoms. Both require urgent recognition and spinal imaging. CES is acute compression of the cauda equina nerve roots, while MSCC is cord/cauda compression due to metastatic cancer. Both can cause permanent neurological damage if missed.
Definitions
Cauda Equina Syndrome (CES)
- Acute or rapidly progressive compression of the cauda equina nerve roots (L2-S5), usually from a large lumbar disc prolapse
- When compressed patient can lose their ability to transmit parasympathetic and somatic signals, leading variable loss of bladder, bowel, sexual, perineal sensory, and bilateral lower-limb function
Metastatic Spinal Cord Compression (MSCC)
- Compression of the spinal cord or cauda equina due to metastatic tumour (vertebral collapse, tumour infiltration, or canal narrowing), causing neurologic dysfunction and risk of permanent paralysis.
★Why Urologists Must Be Vigilant
- Both CES and MSCC often first appear as urinary problems (new retention, loss of bladder sensation, overflow) that can be mistaken for prostatism or UTI.
- CES compresses the S2–S4 roots early, causing neurogenic bladder dysfunction sometimes without back pain; MSCC can do the same, especially in cancer patients.
- Misdiagnosis risks permanent neurological damage, and urologists are well-placed to spot red-flag patterns like painless retention, loss of bladder sensation, or saddle sensory changes.
Causes
CES
occurs when the lumbosacral nerve roots (L2–S5) are compressed.
Main causes:
- Large central lumbar disc prolapse (most common)
- Trauma (fracture/burst injury, post-operative haematoma)
- Infection (epidural abscess, discitis)
- Spinal stenosis (acute on chronic narrowing)
- Primary spinal tumours
- Iatrogenic (post-surgery, post-epidural/spinal anaesthetic haematoma)
MSCC
occurs when the spinal cord or cauda equina is compressed by metastatic cancer.
Main causes:
- Vertebral metastases from: Breast, Prostate, Lung
Mechanisms of compression:
- Vertebral collapse
- Epidural tumour spread
- Paraspinal tumour invading the canal
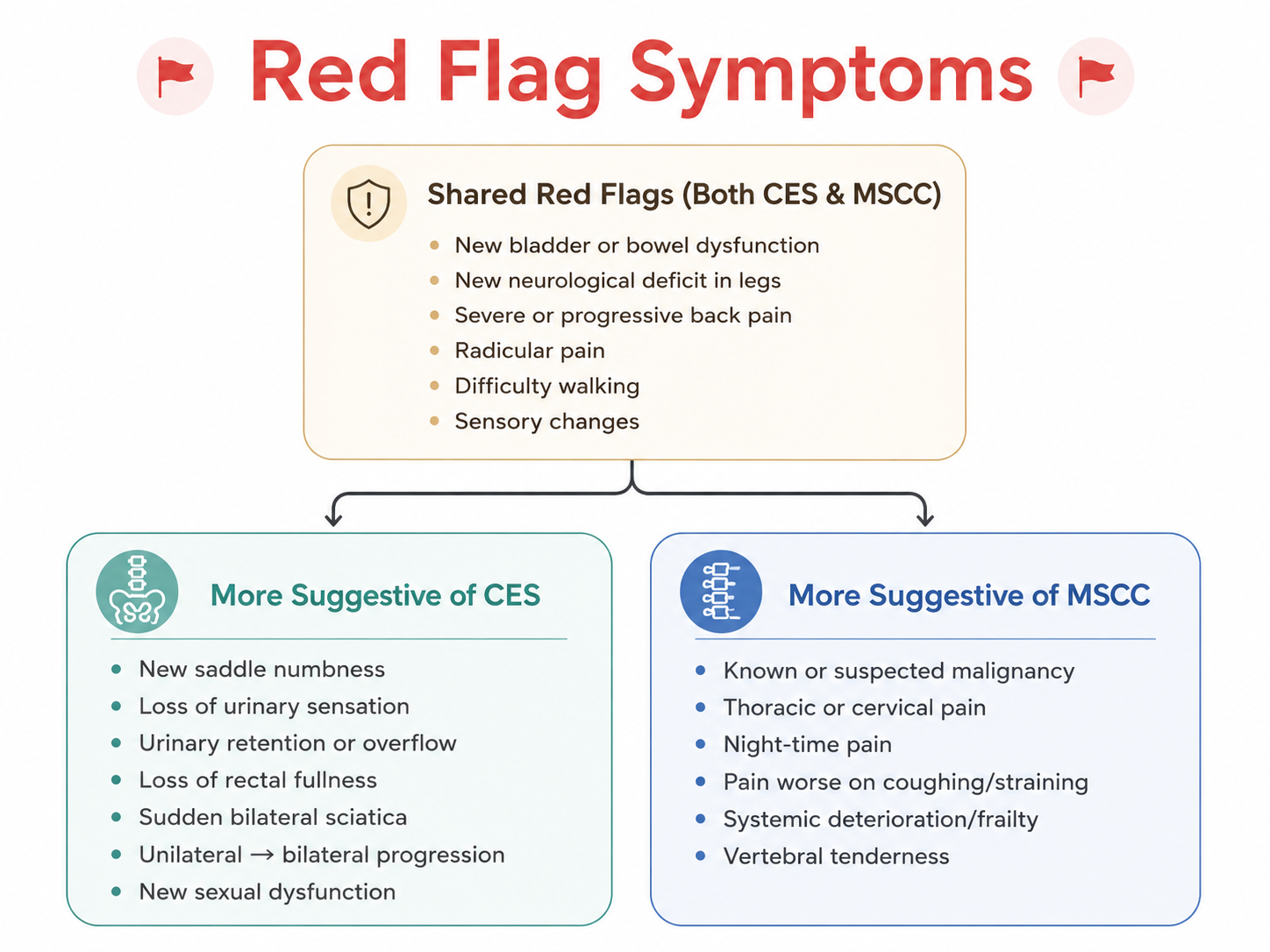
Symptoms
1Pain
- CES: back pain with radiculopathy; may be unilateral or bilateral
- MSCC: 95% present with severe spinal pain—often nocturnal, progressive, or worsened by straining
2Bladder/Bowel/Sexual Function
CES:
- Difficulty initiating urination
- Impaired urinary sensation
- Retention ± overflow
- Loss of rectal fullness
- Bowel incontinence
- Sexual dysfunction (loss of erection/ejaculation/genital sensation)
MSCC: Bladder/bowel dysfunction usually later, associated with cord compromise. May mirror CES symptoms when low lumbar involvement occurs, but usually accompanied by systemic cancer signs
3Neurological
CES:
- Saddle anaesthesia (S2–S5)
- Bilateral sciatica (sudden or evolving)
- Bilateral leg weakness (foot drop, knee extension weakness)
MSCC:
- Limb weakness (often progressive)
- Sensory level
- Gait disturbance
- Upper motor neurone signs (except with conus/cauda involvement)
Examination
1Neurological Exam (Both)
- Lower-limb power: knee extension (L3/4), ankle dorsiflexion (L4/5), ankle eversion (L5)
- Sensory testing: dermatomes including S2–S5 (perineal/saddle region)
- Reflexes & UMN signs: hyperreflexia, clonus, Babinski (more suggestive of MSCC)
- Gait assessment (if safe) to identify functional decline or weakness
- DRE is not routinely necessary, but subjective perianal sensation should be recorded
CES-specific Exam
- Perianal/perineal sensation: ask and/or examine; subjective sensation is acceptable (GIRFT)
- Rectal fullness: ask if reduced or absent
MSCC-specific Exam
- Spinous process tenderness (common in vertebral tumour/collapse)
- Sensory level: thoracic or cervical level change suggests cord involvement
- Upper motor neurone signs: particularly in cord compression (spasticity, clonus)
- Assess overall fitness for transfer: many MSCC patients are frail or systemically unwell
2Bladder assessment
- Post-void residual (PVR) bladder scan:
- <200 mL does not exclude CES
- >200 mL increases likelihood of CES
- >600 mL → catheterise (document sensation + tug)
- Look for painless retention, a key indicator of sacral root dysfunction
MRI & Imaging Timing
- MRI is the test of choice for both CES and MSCC
- CT may assist with bony anatomy, but does not replace MRI
- Do NOT delay imaging for blood tests
CES
- Emergency MRI as soon as possible, ideally within 4 hours of arrival
- MRI focuses on lumbar spine
- MRI confirms compression, but clinical symptoms define CES
MSCC
- Whole-spine MRI within 24 hours if MSCC suspected
- Spine pain + metastasis (no neurology): MRI within 1 week
Emergency Treatment
If you suspect CES or MSCC:
- Order urgent MRI + speak with Radiologist to vet it
- Escalate to spinal/neurosurgical team
- Immobilisation [3 reference]:
- Start if suspected or confirmed MSCC + neurology or spinal instability
- Consider if MSCC or spinal mets + moderate or severe pain associated with movement
- Read more HERE
- Analgesia
- Document exact timing of symptom onset
- Catheterise if retention
- If suspected MSCC → Dexamethasone 16 mg daily + PPI (unless lymphoma suspected or contraindication)
CES - Neurosurgical Treatment
- This is a NEUROSURGICAL EMERGENCY
- Urgent decompression surgery (within 48h, ideally <24h)
- Best outcomes if surgery within 48 hours
- Delay beyond 48h associated with permanent deficit
MSCC - Oncological Treatment
- Dexamethasone 16mg daily (unless lymphoma suspected or contraindicated)
- Radiotherapy is often first-line for MSCC
- Surgery if: single level, good prognosis, radio-resistant
- MDT decision (oncology, neurosurgery, palliative care)
★Urological Involvement
- Urologists may be first to see patient presenting with acute urinary retention
- HIGH INDEX OF SUSPICION needed — always ask about saddle symptoms and bilateral leg symptoms in retention
- Catheterise and document residual volume
- Urgent neurosurgery/spinal referral if CES or MSCC suspected
- Post-operatively: may need long-term catheter or ISC
- Urodynamics may be needed later to assess bladder function recovery
GIRFT guidelines - National suspected cauda equina pathway
The Getting It Right First Time (GIRFT) programme has published a national suspected cauda equina pathway to standardise assessment and management across the UK.
This flowchart guides clinicians from primary care presentation through to post-operative care
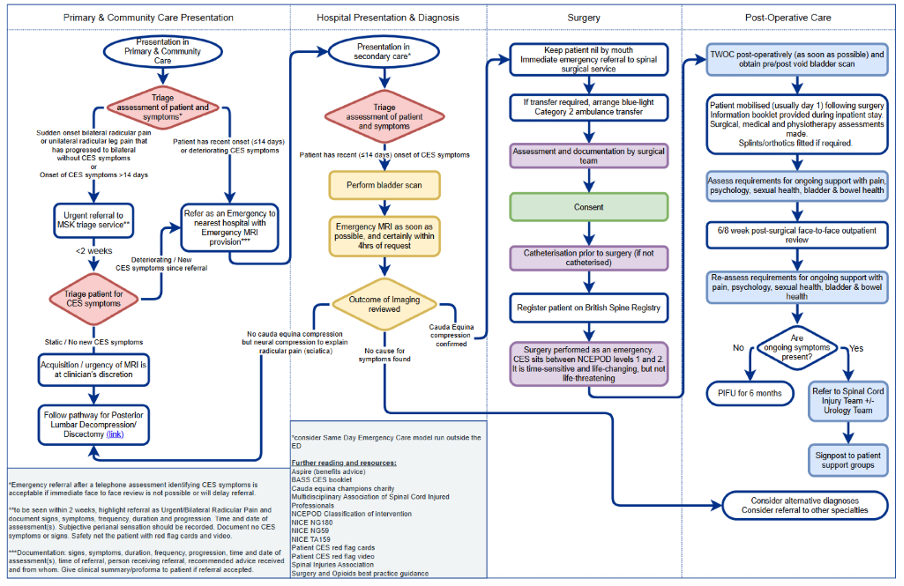
Click image to open full size.
View GIRFT national suspected cauda equina pathway